Learning how to learn brachial plexus anatomy can be a challenging yet rewarding endeavor. This complex network of nerves is crucial for understanding the function and potential dysfunction of the upper limb. At LEARNS.EDU.VN, we’re dedicated to providing you with clear, concise, and engaging resources to master this essential topic, transforming complex anatomy into manageable knowledge. Unlock your potential with effective brachial plexus learning strategies, detailed anatomical guides, and expert insights found at LEARNS.EDU.VN.
1. Understanding the Brachial Plexus: An Overview
The brachial plexus is a complex network of nerves originating in the neck and extending into the axilla, ultimately providing innervation to the upper limb. Mastering its anatomy is crucial for medical professionals, students, and anyone interested in understanding the intricate workings of the human body. Let’s embark on a journey to unravel the complexities of the brachial plexus, making it easier to comprehend and retain.
1.1 What is the Brachial Plexus?
The brachial plexus is a network of nerve fibers that supplies the skin and musculature of the upper limb. It’s responsible for motor and sensory functions in the arm, forearm, and hand. Understanding its structure and function is essential for diagnosing and treating various conditions affecting the upper limb.
1.2 Why is Learning the Brachial Plexus Important?
Learning about the brachial plexus is vital for several reasons:
- Medical Diagnosis: Injuries to the brachial plexus can result in significant functional impairments. A thorough understanding of its anatomy is essential for accurate diagnosis and treatment planning.
- Surgical Procedures: Surgeons operating in the shoulder, axilla, and upper limb regions must have a comprehensive understanding of the brachial plexus to avoid iatrogenic injury.
- Rehabilitation: Therapists use their knowledge of the brachial plexus to design effective rehabilitation programs for patients with nerve injuries.
- Anatomical Knowledge: For students of medicine, physical therapy, and other related fields, the brachial plexus is a key component of anatomical knowledge.
1.3 Key Components of the Brachial Plexus
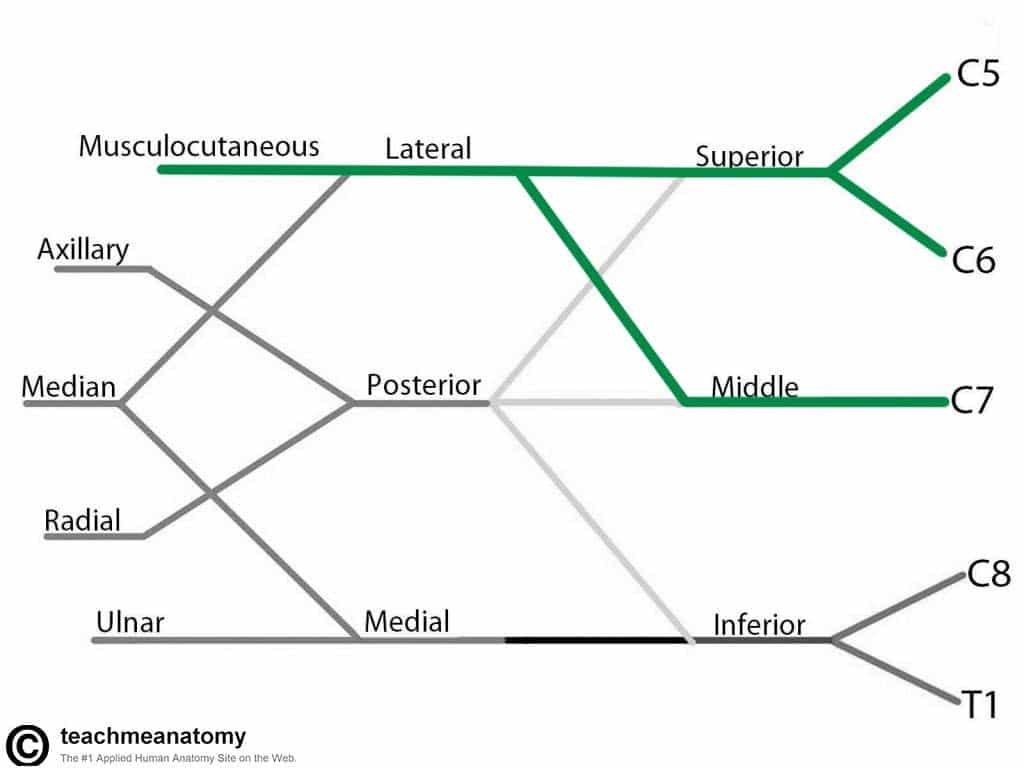
The brachial plexus is traditionally divided into five parts:
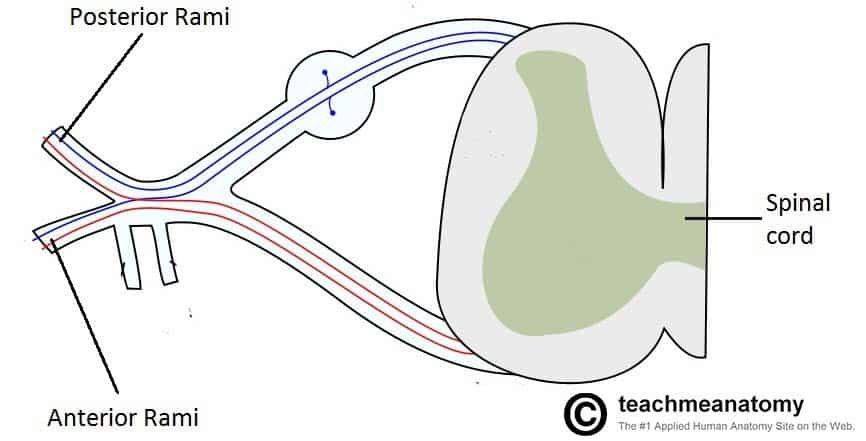
- Roots: The anterior rami of spinal nerves C5, C6, C7, C8, and T1.
- Trunks: The roots merge to form three trunks: superior, middle, and inferior.
- Divisions: Each trunk divides into an anterior and a posterior division.
- Cords: The divisions recombine to form three cords: lateral, posterior, and medial.
- Branches: The cords give rise to the major peripheral nerves of the upper limb.
Mnemonic devices such as “Read That Damn Cadaver Book” can assist in remembering the order: Roots, Trunks, Divisions, Cords, Branches.
1.4 Common Challenges in Learning the Brachial Plexus
Many students find the brachial plexus challenging due to its complexity and the numerous components that need to be memorized. Some common difficulties include:
- Spatial Orientation: Visualizing the three-dimensional arrangement of the nerves can be difficult.
- Memorization: Remembering the origins, pathways, and branches of each nerve requires significant effort.
- Clinical Application: Connecting the anatomy to clinical scenarios can be challenging for beginners.
At LEARNS.EDU.VN, we recognize these challenges and provide targeted strategies and resources to help you overcome them.
2. Effective Learning Strategies for the Brachial Plexus
Mastering the brachial plexus requires a strategic approach that combines various learning techniques. Here are some effective methods to enhance your understanding and retention.
2.1 Visual Learning Techniques
Visual aids are invaluable for understanding the spatial relationships within the brachial plexus.
-
Diagrams and Illustrations: Use labeled diagrams to trace the path of each nerve from its origin to its target muscles and sensory areas. LEARNS.EDU.VN offers a rich collection of high-quality diagrams to aid your learning.
-
3D Models: Interactive 3D models allow you to rotate and explore the brachial plexus from different angles, providing a deeper understanding of its structure. Consider tools like those offered by Visible Body or complete anatomy.
-
Color-Coding: Assign different colors to each component of the brachial plexus (e.g., roots, trunks, divisions) to help differentiate them visually.
2.2 Active Recall and Spaced Repetition
Active recall involves retrieving information from memory rather than passively rereading notes. Spaced repetition is a technique where you review information at increasing intervals.
-
Flashcards: Create flashcards with the name of a nerve on one side and its origin, branches, and function on the other. Use spaced repetition software like Anki to optimize your review schedule.
-
Self-Testing: Regularly test yourself on the material. LEARNS.EDU.VN provides quizzes and practice questions to assess your knowledge.
-
Teach Others: Explaining the brachial plexus to someone else is a great way to reinforce your understanding and identify any gaps in your knowledge.
2.3 Mnemonic Devices and Acronyms
Mnemonics are memory aids that use associations and patterns to help you remember complex information.
-
Roots to Trunks: Use the mnemonic “Robert Taylor Drinks Cold Beer” to remember the order: Roots, Trunks, Divisions, Cords, Branches.
-
Cords to Branches: Use “My Aunt Really Understands Medicine” to remember the branches of the brachial plexus: Musculocutaneous, Axillary, Radial, Ulnar, Median.
2.4 Utilizing Online Resources and Apps
The digital age offers a wealth of resources to support your learning.
- LEARNS.EDU.VN: Our website provides comprehensive articles, diagrams, and quizzes on the brachial plexus.
- YouTube: Channels like Armando Hasudungan and Osmosis offer clear and concise video tutorials on the brachial plexus.
- Anatomy Apps: Apps like Complete Anatomy and Visible Body provide interactive 3D models and detailed anatomical information.
2.5 Hands-On Learning and Dissection
If possible, engage in hands-on learning experiences to solidify your understanding.
- Anatomical Models: Use physical models of the brachial plexus to visualize its structure and relationships.
- Dissection: If you have access to a cadaver lab, dissecting the brachial plexus can provide invaluable insights into its anatomy.
3. Deep Dive into the Components of the Brachial Plexus
Let’s take a closer look at each component of the brachial plexus, providing detailed information and practical tips for understanding them.
3.1 Roots: The Foundation of the Brachial Plexus
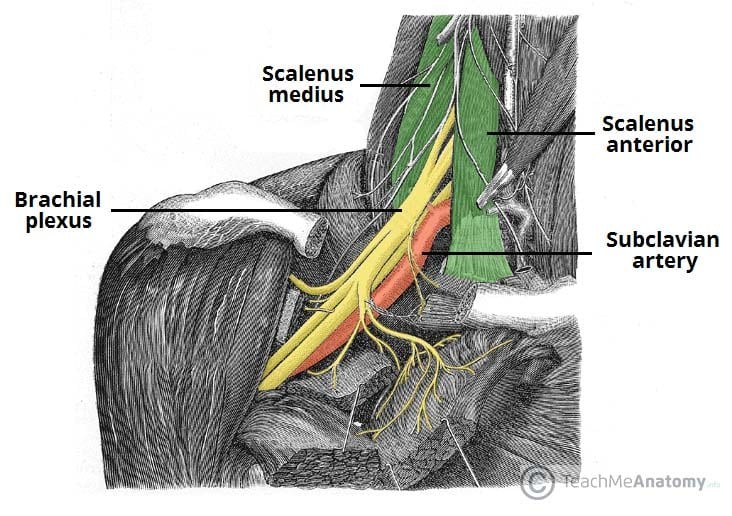
The roots of the brachial plexus are formed by the anterior rami of spinal nerves C5, C6, C7, C8, and T1. These nerves emerge from the spinal cord and pass between the anterior and middle scalene muscles in the neck.
-
Key Points:
- The roots are the starting point of the brachial plexus.
- They are formed by the anterior rami of spinal nerves C5-T1.
- They pass between the anterior and middle scalene muscles.
-
Learning Tip:
- Visualize the spinal cord and the emergence of the nerve roots.
- Understand the relationship of the roots to the scalene muscles.
3.2 Trunks: Convergence of Nerve Roots
The roots of the brachial plexus converge to form three trunks: superior, middle, and inferior.
-
Superior Trunk: Formed by the union of the C5 and C6 roots.
-
Middle Trunk: Formed by the continuation of the C7 root.
-
Inferior Trunk: Formed by the union of the C8 and T1 roots.
-
Key Points:
- The trunks are formed by the convergence of the roots.
- They are located in the lower part of the neck.
- Each trunk represents a different combination of nerve roots.
-
Learning Tip:
- Draw a diagram showing how the roots merge to form the trunks.
- Remember the specific roots that contribute to each trunk.
3.3 Divisions: Anterior and Posterior的分裂
Each trunk divides into an anterior and a posterior division. These divisions represent the next stage in the organization of the brachial plexus.
-
Anterior Divisions: Generally supply the anterior (flexor) compartment of the upper limb.
-
Posterior Divisions: Generally supply the posterior (extensor) compartment of the upper limb.
-
Key Points:
- Each trunk divides into an anterior and a posterior division.
- The divisions represent a functional separation of the nerves.
- Anterior divisions supply flexor muscles, while posterior divisions supply extensor muscles.
-
Learning Tip:
- Understand the functional significance of the anterior and posterior divisions.
- Relate the divisions to the muscles they supply.
3.4 Cords: Recombination of Divisions
The anterior and posterior divisions recombine to form three cords, named according to their position relative to the axillary artery: lateral, posterior, and medial.
-
Lateral Cord: Formed by the anterior divisions of the superior and middle trunks.
-
Posterior Cord: Formed by all three posterior divisions (superior, middle, and inferior trunks).
-
Medial Cord: Formed by the anterior division of the inferior trunk.
-
Key Points:
- The cords are formed by the recombination of the divisions.
- They are named based on their position relative to the axillary artery.
- The cords give rise to the major branches of the brachial plexus.
-
Learning Tip:
- Draw a diagram showing how the divisions combine to form the cords.
- Remember the specific divisions that contribute to each cord.
3.5 Branches: Peripheral Nerves of the Upper Limb
The cords give rise to the major peripheral nerves of the upper limb, which innervate the muscles and skin.
-
Musculocutaneous Nerve: Arises from the lateral cord and innervates the biceps brachii, brachialis, and coracobrachialis muscles.
Roots: C5, C6, C7.
Motor Functions: Innervates the brachialis, biceps brachii and coracobrachialis muscles.
*Sensory Functions: Gives off the lateral cutaneous branch of the forearm, which innervates the lateral half of the anterior forearm, and a small lateral portion of the posterior forearm. -
Axillary Nerve: Arises from the posterior cord and innervates the deltoid and teres minor muscles.
Roots: C5 and C6.
Motor Functions: Innervates the teres minor and deltoid muscles.
*Sensory Functions: Gives off the superior lateral cutaneous nerve of arm, which innervates the inferior region of the deltoid (“regimental badge area”). -
Radial Nerve: Arises from the posterior cord and innervates the triceps brachii and the posterior compartment muscles of the forearm.
Roots: C5 – T1.
Motor Functions: Innervates the triceps brachii, and the muscles in the posterior compartment of the forearm (which are primarily, but not exclusively, extensors of the wrist and fingers).
*Sensory Functions: Innervates the posterior aspect of the arm and forearm, and the posterolateral aspect of the hand. -
Median Nerve: Arises from both the lateral and medial cords and innervates most of the flexor muscles in the forearm and some of the hand muscles.
Roots: C6 – T1. (Also contains fibres from C5 in some individuals).
Motor Functions: Innervates most of the flexor muscles in the forearm, the thenar muscles, and the two lateral lumbricals associated with the index and middle fingers.
*Sensory Functions: Gives off the palmar cutaneous branch, which innervates the lateral part of the palm, and the digital cutaneous branch, which innervates the lateral three and a half fingers on the anterior (palmar) surface of the hand. -
Ulnar Nerve: Arises from the medial cord and innervates some of the flexor muscles in the forearm and most of the intrinsic hand muscles.
Roots: C8 and T1.
Motor Functions: Innervates the muscles of the hand (apart from the thenar muscles and two lateral lumbricals), flexor carpi ulnaris and medial half of flexor digitorum profundus.
*Sensory Functions: Innervates the anterior and posterior surfaces of the medial one and half fingers, and associated palm area. -
Key Points:
- The branches are the terminal nerves of the brachial plexus.
- Each nerve innervates specific muscles and skin areas.
- Understanding the distribution of each nerve is crucial for clinical diagnosis.
-
Learning Tip:
- Create a table listing each nerve and its motor and sensory functions.
- Use diagrams to trace the path of each nerve and its target muscles.
- Relate the nerve distribution to common clinical presentations.
4. Applying Your Knowledge: Clinical Relevance
Understanding the brachial plexus is not just about memorizing anatomy; it’s also about applying that knowledge to clinical scenarios. Let’s explore some common clinical conditions related to the brachial plexus.
4.1 Brachial Plexus Injuries: An Overview
Brachial plexus injuries can result from trauma, compression, or inflammation. These injuries can cause a range of symptoms, from mild weakness to complete paralysis.
-
Types of Injuries:
- Stretching: Occurs when the nerves are stretched beyond their normal limits.
- Compression: Occurs when the nerves are compressed by surrounding structures.
- Avulsion: Occurs when the nerve roots are torn away from the spinal cord.
-
Causes:
- Trauma: Car accidents, sports injuries, and falls.
- Birth Injuries: Erb’s palsy and Klumpke’s palsy.
- Tumors: Can compress or invade the brachial plexus.
- Inflammation: Can cause nerve damage.
4.2 Erb’s Palsy: Upper Brachial Plexus Injury
Erb’s palsy is an injury to the upper roots of the brachial plexus (typically C5-C6). It often occurs during difficult childbirths.
-
Nerves Affected: Musculocutaneous, axillary, and suprascapular nerves.
-
Muscles Affected: Deltoid, biceps brachii, brachialis, and rotator cuff muscles.
-
Clinical Presentation: “Waiter’s tip” position, with the arm adducted, internally rotated, and the forearm pronated.
-
Key Points:
- Erb’s palsy affects the upper roots of the brachial plexus.
- It results in weakness or paralysis of the shoulder and elbow muscles.
- The “waiter’s tip” position is characteristic of this condition.
-
Learning Tip:
- Visualize the muscles affected by Erb’s palsy and their corresponding functions.
- Understand the mechanism of injury and its impact on nerve function.
4.3 Klumpke’s Palsy: Lower Brachial Plexus Injury
Klumpke’s palsy is an injury to the lower roots of the brachial plexus (typically C8-T1). It is less common than Erb’s palsy and can also occur during childbirth.
-
Nerves Affected: Ulnar and median nerves.
-
Muscles Affected: Intrinsic hand muscles.
-
Clinical Presentation: Claw hand deformity, with hyperextension of the metacarpophalangeal joints and flexion of the interphalangeal joints.
-
Key Points:
- Klumpke’s palsy affects the lower roots of the brachial plexus.
- It results in weakness or paralysis of the hand muscles.
- The claw hand deformity is characteristic of this condition.
-
Learning Tip:
- Visualize the muscles affected by Klumpke’s palsy and their corresponding functions.
- Understand the mechanism of injury and its impact on nerve function.
4.4 Thoracic Outlet Syndrome: Compression of the Brachial Plexus
Thoracic outlet syndrome (TOS) is a condition that involves compression of the nerves and blood vessels in the space between the collarbone and the first rib (thoracic outlet).
-
Causes:
- Anatomical abnormalities (e.g., cervical rib).
- Poor posture.
- Repetitive arm movements.
- Trauma.
-
Symptoms:
- Pain in the shoulder and neck.
- Numbness and tingling in the arm and hand.
- Weakness in the arm and hand.
- Swelling of the arm and hand.
-
Key Points:
- TOS involves compression of the brachial plexus and blood vessels.
- It can cause a variety of symptoms in the upper limb.
- Diagnosis and treatment often involve physical therapy and lifestyle modifications.
-
Learning Tip:
- Understand the anatomical structures that can compress the brachial plexus in TOS.
- Relate the symptoms of TOS to the specific nerves and blood vessels affected.
4.5 Diagnostic Techniques for Brachial Plexus Injuries
Several diagnostic techniques are used to evaluate brachial plexus injuries, including:
- Physical Examination: Assessing motor and sensory function in the upper limb.
- Electromyography (EMG): Measuring the electrical activity of muscles to assess nerve function.
- Nerve Conduction Studies (NCS): Measuring the speed of electrical signals along nerves.
- Magnetic Resonance Imaging (MRI): Providing detailed images of the brachial plexus and surrounding structures.
| Diagnostic Technique | Description |
|---|---|
| Physical Examination | Assessment of motor and sensory function to identify areas of nerve damage. |
| Electromyography (EMG) | Measures the electrical activity in muscles, helping to determine if muscles are responding correctly to nerve signals. |
| Nerve Conduction Studies (NCS) | Measures the speed at which electrical signals travel along nerves, identifying areas where nerve conduction is slowed or blocked. |
| Magnetic Resonance Imaging (MRI) | Provides detailed images of the brachial plexus and surrounding tissues, helping to identify structural abnormalities, tumors, or other conditions that may be affecting the nerves and tissues. |
5. Advanced Learning Techniques and Resources
To deepen your understanding of the brachial plexus, consider exploring advanced learning techniques and resources.
5.1 Cadaver Dissection
If you have the opportunity to participate in cadaver dissection, it can provide invaluable insights into the anatomy of the brachial plexus. Dissection allows you to visualize the three-dimensional arrangement of the nerves and their relationships to surrounding structures.
-
Tips for Effective Dissection:
- Use a detailed dissection guide to help you identify the various components of the brachial plexus.
- Take your time and carefully separate the nerves from the surrounding tissues.
- Use anatomical atlases and diagrams to confirm your identifications.
- Work with a group of classmates to discuss and learn from each other.
5.2 Clinical Case Studies
Studying clinical case studies can help you apply your knowledge of the brachial plexus to real-world scenarios. Case studies often present a patient’s history, physical examination findings, diagnostic test results, and treatment plan.
-
Benefits of Studying Case Studies:
- Improve your diagnostic skills.
- Enhance your understanding of the clinical presentation of brachial plexus injuries.
- Develop your ability to formulate treatment plans.
- Learn from the experiences of other healthcare professionals.
-
Resources for Finding Case Studies:
- Medical journals (e.g., Journal of Bone and Joint Surgery, American Journal of Physical Medicine & Rehabilitation).
- Online case study databases.
- Textbooks on physical medicine and rehabilitation.
5.3 Research Articles
Reading research articles can help you stay up-to-date on the latest advances in the understanding and treatment of brachial plexus injuries. Research articles often present new findings from clinical trials, anatomical studies, and biomechanical analyses.
-
Tips for Reading Research Articles:
- Start by reading the abstract to get an overview of the study.
- Pay attention to the methods section to understand how the study was conducted.
- Carefully review the results section to understand the findings of the study.
- Read the discussion section to understand the authors’ interpretation of the findings.
- Consult with experts or mentors to clarify any questions or uncertainties.
-
Resources for Finding Research Articles:
- PubMed.
- Google Scholar.
- Medical databases (e.g., Ovid, Web of Science).
5.4 Expert Interviews and Lectures
Listening to interviews and lectures from experts in the field can provide valuable insights into the brachial plexus and its clinical relevance. Experts can share their experiences, insights, and perspectives on the diagnosis, treatment, and rehabilitation of brachial plexus injuries.
-
Benefits of Listening to Experts:
- Gain a deeper understanding of the complexities of the brachial plexus.
- Learn about cutting-edge research and clinical practices.
- Hear real-world examples of brachial plexus injuries and their management.
- Network with experts and mentors in the field.
-
Resources for Finding Expert Interviews and Lectures:
- Medical conferences and seminars.
- Online medical education platforms.
- Podcasts and video channels featuring medical experts.
5.5 Virtual Reality and Augmented Reality
Virtual reality (VR) and augmented reality (AR) technologies are increasingly being used in medical education and training. VR and AR can provide immersive and interactive experiences that enhance your understanding of the brachial plexus.
-
Benefits of VR and AR:
- Visualize the brachial plexus in three dimensions.
- Interact with the nerves and surrounding structures in a virtual environment.
- Practice clinical skills in a safe and controlled setting.
- Improve your spatial reasoning and anatomical knowledge.
-
Resources for VR and AR Learning:
- VR anatomy apps and platforms.
- AR anatomy textbooks and guides.
- Medical simulation centers that offer VR and AR training.
6. Case Studies: Real-World Applications
Applying your knowledge to real-world scenarios is crucial for solidifying your understanding of the brachial plexus. Let’s explore a few case studies to illustrate how anatomical knowledge translates into clinical practice.
6.1 Case Study 1: A 25-Year-Old Athlete with Shoulder Weakness
- Patient Presentation: A 25-year-old male presents with weakness in his right shoulder following a football injury. He reports difficulty lifting his arm overhead and experiences pain during abduction.
- Physical Examination: Examination reveals weakness in shoulder abduction and external rotation. Sensory examination is normal.
- Diagnostic Findings: MRI reveals a brachial plexus injury affecting the upper trunk (C5-C6).
- Diagnosis: Upper brachial plexus injury (Erb’s palsy).
- Treatment: Physical therapy to strengthen the affected muscles and improve range of motion.
6.2 Case Study 2: A Newborn with Erb’s Palsy
- Patient Presentation: A newborn is noted to have limited movement in her left arm following a difficult vaginal delivery. The arm is held in adduction and internal rotation, with the forearm pronated.
- Physical Examination: Examination reveals weakness in shoulder abduction, external rotation, and elbow flexion. Sensory examination is intact.
- Diagnostic Findings: Clinical presentation consistent with Erb’s palsy.
- Diagnosis: Erb’s palsy.
- Treatment: Gentle range-of-motion exercises and physical therapy to prevent contractures and promote nerve regeneration.
6.3 Case Study 3: A Patient with Thoracic Outlet Syndrome
- Patient Presentation: A 45-year-old female presents with pain, numbness, and tingling in her right arm and hand. She reports that her symptoms are aggravated by overhead activities and repetitive arm movements.
- Physical Examination: Examination reveals tenderness in the supraclavicular region and a positive Adson’s test.
- Diagnostic Findings: Nerve conduction studies reveal slowing of nerve conduction across the thoracic outlet.
- Diagnosis: Thoracic outlet syndrome.
- Treatment: Physical therapy to improve posture, strengthen the shoulder muscles, and stretch the pectoral muscles.
7. Maintaining Your Knowledge: Ongoing Learning and Review
Learning the brachial plexus is an ongoing process that requires regular review and reinforcement. Here are some strategies to help you maintain your knowledge over time.
7.1 Regular Review Sessions
Schedule regular review sessions to revisit the anatomy of the brachial plexus. Use a variety of resources, such as diagrams, flashcards, and online quizzes, to reinforce your understanding.
7.2 Clinical Practice
Applying your knowledge in clinical practice is one of the best ways to maintain your understanding of the brachial plexus. As you encounter patients with brachial plexus injuries, take the time to review the anatomy and pathophysiology of their conditions.
7.3 Continuing Education
Attend continuing education courses and conferences to stay up-to-date on the latest advances in the diagnosis and treatment of brachial plexus injuries. These events often feature expert speakers, case presentations, and hands-on workshops.
7.4 Teach Others
Teaching others about the brachial plexus is a great way to reinforce your own understanding. By explaining the anatomy and clinical relevance of the brachial plexus to students, colleagues, or patients, you will strengthen your knowledge and identify any gaps in your understanding.
7.5 Utilize Online Resources
Take advantage of online resources, such as LEARNS.EDU.VN, to review the anatomy of the brachial plexus and stay current on the latest research and clinical practices. Our website offers a wealth of articles, diagrams, and quizzes to support your ongoing learning.
8. Summary of Key Learning Strategies
To recap, here are the key strategies for effectively learning the brachial plexus:
- Visual Learning: Use diagrams, 3D models, and color-coding to visualize the anatomy of the brachial plexus.
- Active Recall: Test yourself regularly using flashcards, quizzes, and self-testing.
- Mnemonic Devices: Use mnemonics to remember the order of the roots, trunks, divisions, cords, and branches.
- Online Resources: Take advantage of online resources, such as LEARNS.EDU.VN, to supplement your learning.
- Hands-On Learning: Participate in cadaver dissection or use anatomical models to visualize the anatomy of the brachial plexus.
- Clinical Relevance: Apply your knowledge to clinical scenarios by studying case studies and understanding the clinical presentation of brachial plexus injuries.
- Ongoing Learning: Maintain your knowledge by scheduling regular review sessions, attending continuing education courses, and teaching others about the brachial plexus.
9. Frequently Asked Questions (FAQs)
9.1 What are the roots of the brachial plexus?
The roots of the brachial plexus are the anterior rami of spinal nerves C5, C6, C7, C8, and T1.
9.2 What are the trunks of the brachial plexus?
The trunks of the brachial plexus are the superior, middle, and inferior trunks.
9.3 What are the cords of the brachial plexus?
The cords of the brachial plexus are the lateral, posterior, and medial cords.
9.4 What are the major branches of the brachial plexus?
The major branches of the brachial plexus are the musculocutaneous, axillary, radial, median, and ulnar nerves.
9.5 What is Erb’s palsy?
Erb’s palsy is an injury to the upper roots of the brachial plexus (C5-C6), resulting in weakness or paralysis of the shoulder and elbow muscles.
9.6 What is Klumpke’s palsy?
Klumpke’s palsy is an injury to the lower roots of the brachial plexus (C8-T1), resulting in weakness or paralysis of the hand muscles.
9.7 What is thoracic outlet syndrome?
Thoracic outlet syndrome is a condition that involves compression of the nerves and blood vessels in the space between the collarbone and the first rib.
9.8 How are brachial plexus injuries diagnosed?
Brachial plexus injuries are diagnosed through physical examination, electromyography (EMG), nerve conduction studies (NCS), and magnetic resonance imaging (MRI).
9.9 How are brachial plexus injuries treated?
Brachial plexus injuries are treated with physical therapy, occupational therapy, pain management, and, in some cases, surgery.
9.10 Where can I find more resources on the brachial plexus?
You can find more resources on the brachial plexus at LEARNS.EDU.VN, medical textbooks, online anatomy resources, and medical journals.
10. Conclusion: Empowering Your Learning Journey with LEARNS.EDU.VN
Mastering the brachial plexus is a challenging but achievable goal. By utilizing effective learning strategies, engaging with high-quality resources, and applying your knowledge to clinical scenarios, you can develop a deep and lasting understanding of this complex anatomical structure.
Remember, the key to success is consistent effort, active engagement, and a willingness to seek help when needed. Whether you’re a medical student, a healthcare professional, or simply an anatomy enthusiast, LEARNS.EDU.VN is here to support you on your learning journey.
Ready to take your understanding of the brachial plexus to the next level? Visit LEARNS.EDU.VN today to explore our comprehensive collection of articles, diagrams, quizzes, and other valuable resources. Let us help you unlock your full potential and achieve your learning goals.
For more information, please contact us at:
Address: 123 Education Way, Learnville, CA 90210, United States
WhatsApp: +1 555-555-1212
Website: learns.edu.vn
